 When should a chest xray be repeated during the dwell time for any central vascular access devices (CVAD)? This is a frequent question for many nurses and facilities and it involves several different scenarios. There is a risk of radiation exposure, albeit small, from a routine chest xray. Reducing their use will reduce this exposure along with decreasing costs. However, there will be clinical situations when the benefits outweigh these risks. When a new patient with a PICC or implanted port is admitted to your facility or agency, the first option is to check documentation of the original tip location at the time of insertion. But there will be many times when this information is not available. Do you know about tip location practices in other facilities or agencies in your area? Some may still be using the old “midclavicular” tip location for PICCs with the inserted catheter length based exclusively on external measurement. Some practitioners may not understand or acknowledge the importance of tip location at the cavoatrial junction, leaving the tip high in the superior vena cava. This means the first reason would be a suboptimal tip location on insertion. The second reason would be clinical signs and symptoms of a malfunction or malposition which can occur at any time for many reasons. Clinical assessment of all CVADs is on ongoing process while the patient is under your care. Signs and symptoms are outlined in an evidence-based list in the 2016 Infusion Therapy Standards of Practice and includes:
 For many years, we have overlooked the infection risk associated with peripheral IV (PIV) catheters while focusing exclusively on infection risk associated with central vascular access devices. Our attention must include both! While there is no doubt that published rates of central line associated bloodstream infection (CLABSI) were far too high, we must take a closer look at the rates of BSI that are associated with PIV catheters as well. Unfortunately, there is very little prospective data on actual PIV-BSI rates. There are 2 unique studies on Staphylococcus aureus BSI that used retrospective data to analyze the problem. These studies reported similar processes and outcomes. Both studies used medical records to identify patients with S. aureus BSI and correlated blood culture results with clinical data. Trinh, et.al, reported 24 cases of S. aureus BSI related to PIV catheters. They reported these patients to be more likely to have the PIV inserted in the emergency department or outside the hospital and to have the PIV placed in the antecubital fossa. Of all S. aureus BSI, 12% were caused by PIV catheters. Using this data and data on all US hospital adult discharges, these researchers estimated that as many as 10,000 PIV-BSIs from S. aureus alone happen in US hospitals. Austin, et.al, reported 34 of 445 (7.6%) of all S. aureus BSI were related to thrombophlebitis at a PIV catheter site. The length of the bacteremic period was longer in patients with PIV-BSI, primarily caused by methicillin-resistant S. aureus BSI. Most cases were caused by PIV catheters inserted in the proximal forearm and antecubital fossa. Also, most cases were due to thrombophlebitis at old PIV sites. No guidelines recommend frequent monitoring of previous PIV catheter sites for developing or worsening signs and symptoms of thrombophlebitis, however this study indicates the necessity for monitoring sites after PIV removal. The bottom line is the need for careful aseptic technique with each PIV catheter insertion. Don’t use veins of the antecubital fossa. One or two swipes on the skin with an alcohol pad is not sufficient. Touching the prepped site with gloved fingers can only be done when wearing sterile gloves. All methods of infection prevention must be used. Hospitals are no longer reimbursed for treating infections associated with any type of vascular access device, including PIV-BSI. Strict attention to PIV catheter insertion and maintenance is just as important as the attention we now give to central VADs. Short Peripheral Intravenous Catheters and Infections Trinh, T. T., Chan, P. A., Edwards, O., Hollenbeck, B., Huang, B., Burdick, N., . . . Mermel, L. A. (2011). Peripheral Venous Catheter-Related Staphylococcus aureus Bacteremia. Infection control and hospital epidemiology: the official journal of the Society of Hospital Epidemiologists of America, 32(6), 579. Austin, E. D., Sullivan, S. B., Whittier, S., Lowy, F. D., & Uhlemann, A.-C. (2016). Peripheral intravenous catheter placement is an underrecognized source of Staphylococcus aureus bloodstream infection. Paper presented at the Open forum infectious diseases. Online Course Updated - Peripheral IV Therapy in Adults One of our most popular courses has been updated with content that incorporates the 2016 Infusion Therapy Standards of Practice.
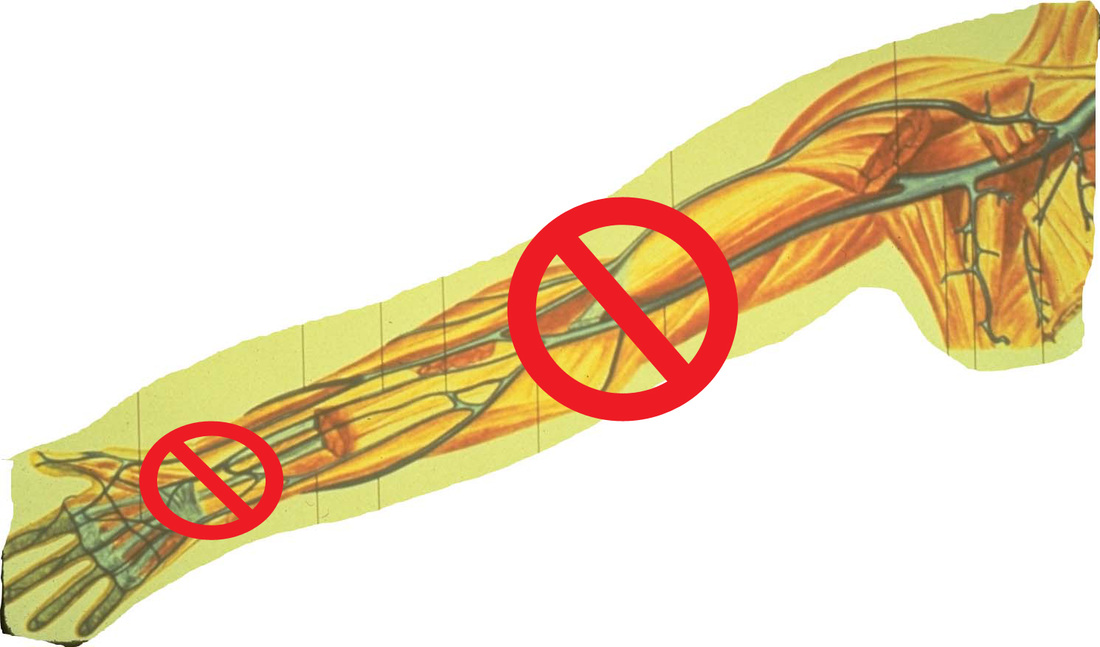
Start out on the right track with this basic course. If you are new to IV therapy, this course will provide the needed information about all steps in process of patient assessment, planning what is needed, performing the procedures and assessing the outcomes. Click here to learn more! 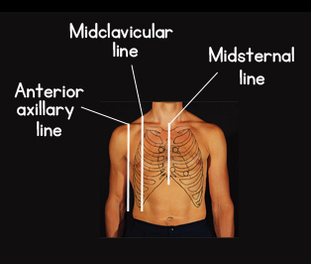 Were you taught to use the axillary lines to determine the tip location for a midline catheter? If so, you need to learn a better method as these lines are nowhere near the appropriate location for the tip of a midline catheter. According to the 2016 Infusion Therapy Standards of Practice, a midline catheter is defined as “a catheter inserted into the upper arm via the basilic, cephalic, or brachial vein, with the internal tip located at or near the level of the axilla and distal to the shoulder.” The axilla is the armpit and this tip location describes placement in the upper arm. A midline catheter must remain in the upper extremity for adults and should never go into the shoulder or chest area. There are 3 axillary lines used for guidance on many procedures like thoracentesis and for placement of various ECG leads. Look at the drawing and notice that all axillary lines are on the chest and do not involve the arm. The anterior axillary line would be the closest to a midline tip location, however using this axillary line would put the midline tip location directly in the shoulder where joint motion will lead to catheter complications. The midclavicular line was the tip location of a midclavicular catheter, however studies in the late 1990’s showed that tip location to have a greater risk of vein thrombosis. For this reason, the INS Standards have never included the midclavicular tip location. To achieve the midline tip location as defined by the INS Standards, place your index finger in the patient’s armpit and bring your thumb around the circumference of the upper arm at that level. This is the correct midline catheter tip location. Choose your insertion site and measure between these 2 points. Insert that length of catheter and you will have a correctly placed midline catheter meeting the definition in the national standards. For clinicians with a bad experience with midline catheters, could this be the reason for their failure? 
 Twas the night before Christmas, and all through the ward, Not a patient was stirring, not a thing to record. The charts were all placed in their slots with great care, In hopes that the doctors would leave them right there. I’d complete my rounds, all the meds and re-starts, Hung three units of blood, and restocked all the charts. When far down the hall, there arose such a clatter, I sprang from the desk to see what was the matter. Away down the hall, I flew like a flash, Rounded the corner, and met with a crash A jolly old man, all covered with snow With a round little belly and cheeks all aglow. “What are you doing here?”, I exclaimed in surprise, As he twinkled at me with his fat little eyes. “Visiting hours were over at eight. It is now after twelve. You are much, much too late.” “Nurse, don’t you know me?”, he said with a smile. “And now that I’m here, can’t I stay for a while?” “I’m afraid I don’t know you”, I exclaimed quite irate. The confusion was such I’d forgotten the date. “But nurse, I have come such a long way” he said “And I couldn’t show up until all were in bed.” “Your excuses are slim and this you must know. Rules are made to be kept; I must ask you to go.” For answer he lifted a sack from his back, Put it down on the floor and began to unpack. More RN’s and LPN’s with infusion experience, I knew it would brighten the entire team’s spirits! Other gifts followed. He had them right there. All the things that were needed for the good patient care. For each of the doctors, a smiling machine, So each could look pleasant, although he felt mean. For each of the nurses, A SALARY RAISE!!!! Saying tell them for me dedication still pays. The best of all gifts, he then pulled out with glee, For each patient, the right VAD! Then I saw that the man I had almost thrown out, Looked very familiar, as he turned about. And I asked him to stay, “Please don’t go!” I grew bolder. But he finished his job, putting his bag on his shoulder. He sprang to his sleigh waiting there on the roof. With eight tiny reindeer, the ultimate proof, Of just who he was and as he flew out of sight, “Merry Christmas” he called, and “God Bless you this night.” Feel Free to Download and use how you see fit!
We will be back in January with announcements about new online courses and video conferences!
Merry Christmas! - Lynn and Megan 
 Can the dressing on a tunneled PICC be eliminated after the tunnel is “healed”? The short answer is NO!
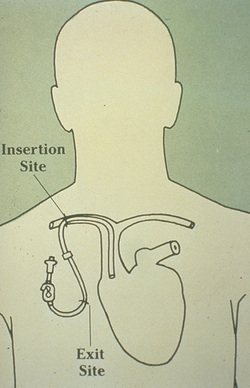
The practice of putting in a PICC using a subcutaneous tunnel seems to be growing. Separating the venipuncture site from the skin exit site may have benefits such as moving the exit site out of the area of neck motion and possible reduction in bloodstream infection from skin organisms, although the evidence supporting infection reduction is not strong. A small size PICC inserted in the jugular vein offers the benefits of bypassing the subclavian vein, a site with higher risk of vein thrombosis. This may be beneficial in -renal failure patients where axillo-subclavian thrombosis can present significant concerns. But don’t confuse a PICC inserted with a short subcutaneous tunnel with a tunneled cuffed catheter (e.g., Hickman®, Broviac®). The subcutaneous tunnel for a PICC is much shorter than the subcutaneous tunnel for a tunneled cuffed CVAD. A tunneled cuffed CVAD has a cuff made of a rough material encircling the outer lumen of the catheter. This cuff is positioned several centimeters away from the skin exit site usually in the middle of the chest. The subcutaneous tissue grows into this cuff causing a mechanical barrier to the migration of skin microorganisms into the bloodstream. It also adds a form of stabilization to prevent dislodgement of the CVAD. A tunneled PICC usually does NOT have this cuff encircling the catheter. Long-term hemodialysis catheters also have this subcutaneous cuff. I am not certain how many brands of PICCs are made with this subcutaneous cuff, however I don’t think there are many. A question I recently received asked about no dressing on a tunneled PICC after it has “healed”, citing the statement in the INS Standard. The statement from the standard on dressing changes is, “When the subcutaneous tunnel is well-healed, consideration may be given to no dressing with a tunneled, cuffed CVAD.” (page S83) It specifically states a tunneled, cuffed CVAD, and this does not apply to PICCs. This statement applies to the time required for the subcutaneous tissue to grow into the cuff. That time varies with each person and depends upon many factors. Once again, most PICCs are not made with these cuffs and a stabilization device and a dressing is required for all PICCs. Skin irritation and inflammation should be prevented by using a skin barrier solution from the very first dressing. This solution (e.g., Skin-Prep®, Cavilon®) are solutions to prevent this irritation, but they are not designed to heal the skin after the irritation is present. Medical adhesive related skin injury (MARSI) is discussed in several standards and the use of this barrier solution is strongly recommended.  CVAD Tip Migration  CVAD Dislodgment A common problem continues to be raised – the absence of information about the original tip location for a PICC when the patient is transferred to another venue of care, especially if multiple transfers are involved. For instance, the PICC is placed while the patient is in the hospital. He is then transferred to a rehabilitation or skilled nursing facility for a period of time and is then transferred home and admitted to a home care agency. No information is provided to the home care agency about the original tip location, or any change in the external measurements.
How should the PICC be used until the original documentation can be obtained? Will it be possible to obtain the original information? Should administration of vesicants and non-vesicants be managed the same way? Without the original documentation, should the PICC be removed with the patient in the home or should the patient be sent to the hospital or practitioner’s office for removal? While a PICC may be the most common CVAD used in these situations, the standard of practice for tip location applies to all CVADs. As we all know, information about the original tip location should go with the patient with each transfer but we know that does not always happen. Additionally, a tunneled cuffed catheter or implanted port may have been inserted months or even years before admission to the current home care company. So there are many situations where the original tip location will not be known. But remember this documentation was only for the location of the CVAD tip at insertion. Many factors can lead to CVAD tip migration during the dwell time, including physical activity, heaving lifting, ventilation, congestive heart failure, or anything that changes intrathoracic venous pressure. Although specific data on the frequency of malposition is not available, patients that have been receiving physical therapy in a rehabilitation program could easily have changes in the tip location. This may happen more frequently if the original tip location was sub-optimal in the mid to upper superior vena cava. Tip migration means that only the CVAD tip is moving and the external segment of the catheter remains unchanged. The tip could migrate to the jugular vein, the opposite subclavian vein, or any number of small tributary veins. Tip migration is sporadic and unpredictable. Dislodgment is a change in the length of the external catheter, which also means that the tip location is retracted by that same distance. These are just 2 examples of malposition but this could also include the catheter tip eroding through the vein wall or cardiac wall, formation of a fistula between an artery and vein or other structures such as the trachea. Before infusing through any CVAD, a complete assessment is necessary. This goes way beyond reliance on information about the original tip location. In addition to assessing for a blood return from each lumen, you should also include flushing to detect difficulty or resistance; changes in blood pressure, heart rate, and/or respiratory rate; any type of pain, discomfort, and/ or presence of edema in the back, neck, shoulder, or chest; complaints of hearing a running stream on the side of the CVAD insertion; and neurological problems like paresthesia. Any problem found during this assessment means the CVAD should not be used until a diagnostic test can be done to determine the cause of the problem. The presence of a blood return that is the color and consistency of whole blood and the absence of all other signs or symptoms of a complication indicates the CVAD can be used. I would apply the same assessment to vesicants and non-vesicants. Although a vesicant has the potential to cause tissue damage for a variety of reasons, a non-vesicant can also cause tissue damage due to compression from the volume infused. Also remember that a vesicant causes the damage OUTSIDE the vein but vein thrombosis is quite common with intravascular malposition. Removal of a PICC or other percutaneous CVAD in the home is routinely done and the nurse may not know the exact location of the tip. If there is a change in how the catheter is functioning or some other complication, it might be wise to have the patient return to a clinic or practitioner office for removal. Each situation requires a thorough assessment and application of critical thinking skills. While the original tip location information is important to have, it really provides no information about where the tip is located weeks or months into the dwell time and use of the catheter. You must rely on your assessment of the patient and the CVAD. When signs and symptoms of malposition are present, a diagnostic test such as a chest radiograph or ultrasound is needed. 
Many questions still arise about the need for informed consent for a midline catheter. My answer is Yes and No! To ensure that all who read this understands my thoughts, I need to emphasize the definition of informed consent from the 2016 INS Standards of Practice:
“A person’s voluntary agreement, based upon adequate knowledge and understanding of relevant information, to participate in research or to undergo a diagnostic, therapeutic, or prentice procedure” Standard #9 provides more details on informed consent, emphasizing this as an educational process based on shared decision-making. This standard does not provide a list of procedures that require informed consent. If you are thinking of “informed consent” as the signature on a piece of paper, the answer is either yes or no for a midline catheter insertion based on the direction of your risk management department. They will know about any applicable state laws regarding informed consent. Risk management’s decision should be included in your policy and procedure for midline catheter insertion. I would also encourage you to broaden your thinking about informed consent. This is an educational process that ends with a signature on a piece of paper but the patient’s adequate knowledge comes from what they are taught, preferably by the midline inserter who would have the most current and accurate knowledge about this procedure. The educational component of the informed consent process is always required for all procedures and all patients in all situations. Even if your facility does not require a signature on that consent form, you should still be educating the patient about the catheter, why they need it, what the procedure will entail, risks, benefits, and complications. If a signed consent form is required, the education must also include alternatives to the proposed midline catheter. So, the possible answers are
Both approaches still require patient education. The INS standard on informed consent includes 9 criteria for appropriate education for the patient’s age and level of health literacy. Please check out this standard for the details.  Yes, it does exist! After a peripheral catheter is removed, phlebitis can develop with the same signs and symptoms as when the catheter was still in the vein – redness, pain, swelling, a palpable cord and purulent drainage. In the photo, the long red streak up the arm is an example of post infusion phlebitis from a contrast agent used for an MRI. This happened to a friend, so I am not sure about which contrast was actually used. When she returned the next day to the Radiology Department asking about her arm, the response was one of denial about the venipuncture or contrast injection being the cause of this red streak up her arm. She ended up in an emergency department receiving doses of I.V. antibiotic and steroids and she responded well. A recent study documented post-infusion phlebitis in 59 of 5907 short peripheral catheters (1.8%) in 3283 patients at 48 hours after catheter removal. Phlebitis at the time of catheter removal was present in only 15 of these 59 patients (25%), with the remaining 75% developing the phlebitis after catheter removal. This calls for written information explaining to the patient and family about observing for signs and symptoms at and near the insertion site. This information should also include any actions they should take and which healthcare practitioner they should contact with any problem or question. You just never know when this red streak could be the first sign of a bacterial phlebitis that becomes a bloodstream infection. Reference Webster J, McGrail M, Marsh N, Wallis MC, Ray-Barruel G, Rickard CM. Postinfusion Phlebitis: Incidence and Risk Factors. Nursing research and   The specialty of infusion nursing is high on the list of specialties in demand and expected to grow by double digits from now until 2022. This article from Scrubs magazine reported the salary for an infusion therapy nurse was $79,139 in 2015. Click here to read the entire article. This current high demand and project growth means that more nurses will need to expand their knowledge and skills in infusion therapy. We have been offering online continuing education courses in this specialty for many years and plan to continue this program for many years to come. We are currently in the process of making an in-depth assessment of our program and need to hear your thoughts. Currently we are working on updating the basic courses to incorporate the 2016 INS Standards of Practice. This includes Peripheral IV Therapy and Central Vascular Access Devices. We also offer 5 advanced courses but I am certain there are other topics that can and should be covered. Additionally, more patient care, including infusion therapy, is being shifted from the hospital into alternative sites such as skilled nursing facilities and ambulatory clinics. Even if you don’t think of yourself as an infusion nurse, you still need the most recent information and highest level of skills if you are responsible for safe delivery of any type of infusion therapy. Please help us meet your needs by emailing megan1@hadawayassociats.com or replying in the comment section with your thoughts and ideas
My phone continues to ring with calls from attorneys about extravasation lawsuits. Over the past 20 years, I have been an expert on about 700 cases, with the majority having seriously bad outcome from extravasation. It is time to explore some myths that many nurses have about peripheral I.V. sites and the correct administration of vesicant I.V. medications.
Myth #1 – Infiltration and extravasation are the same thing. Facts – The Infusion Nurses Society defines infiltration as the inadvertent administration of non-vesicant solution or medication into the surrounding tissue. Extravasation is the inadvertent administration of a vesicant medication into the tissue around the vein. A vesicant is any solution or medication capable of causing tissue damage when it enters tissue surrounding the vein. Myth #2 – It is best to use the veins of the hand, wrist or antecubital fossa because those are the most visible veins. Facts – Many studies now show that greater number and severity of I.V. complications occur in these areas of joint flexion. The Infusion Therapy Standards of Practice have stated for many years to avoid using these veins. They are NOT safe locations for any I.V. catheter. Learn to palpate for veins in the forearm and choose sites that are naturally splinted by the bones of the arm. Myth #3 – An armboard is not necessary and should not be used because it is considered to be a restraint for the patient. Facts – An armboard is NOT a restraint because it’s main purpose is for patient safety and prevention of complications. The Infusion Therapy Standards of Practice calls for the use of armboards, correctly applied, when your only choice is a vein in or close to an area of joint flexion. If veins in these sites must be used, the joint must be supported with an armboard to prevent erosion of the catheter through the vein wall. Think about the patient’s movement with that hand or arm as this leads to vein damage and extravasation. Myth #4 – Only antineoplastic chemotherapy drugs for cancer patients are vesicants and I don’t give those drugs. Facts – There are numerous non-cancer drugs given very frequently that are vesicants including calcium chloride and calcium gluconate, high concentration of potassium chloride, promethazine, phenytoin, sodium bicarbonate, high concentrations of dextrose, contrast agents in radiology, and vancomycin and nafcillin. These drugs can be given in numerous healthcare settings and can pose significant risk to your patients. Myth #5 – If my employer thought I needed to know about these drugs and how to give them, they would provide inservice training. Fact – This is an issue of competency and your professional responsibility to become competent and maintain your competency. It is your employer’s responsibility to assess and validate your competency. This means that you must perform peripheral I.V. catheter insertion according to the Infusion Therapy Standards of Practice which includes site selection for that catheter. This document also states, “The clinician reviews information regarding the prescribed medication/solution including indications, dosing, acceptable infusion routes/rates, compatibility data, and adverse/side effects for appropriateness prior to administration.” This is basic nursing responsibility. If the prescribed I.V. medication is a vesicant, it is the nurse’s responsibility to know this and to know how to safely give it. This means assessing the site every 5 to 10 mLs of infusion which includes checking for a blood return. If your pharmacy mixes a vesicant medication to be infused over a couple of hours, this puts an extra burden on you to remain with the patient, doing these frequent assessment, which must include the presence of a blood return before, during, and after administration. The goal is to stop the infusion immediately at the very first sign of a problem. This could be patient complaints of burning, lack of a blood return or any other compliant at the site. The Bottom Line-- As a nurse, your actions and interventions are to protect your patients. If you do not have the appropriate knowledge, critical thinking, and psychomotor skills to safely administer a vesicant I.V. medication, then you must gain these skills or seek help from another nurse to give the drug. It is your responsibility not that of your employer. I know this post sounds stern and harsh, but I am overwhelmed by seeing horrible, life-altering outcomes from I.V. extravasation injury. Protect your patient, your employer and yourself by safe infusion practices as outlined in the Infusion Therapy Standards of Practice. Ensure that your current policies and procedures incorporate these standards from the recent 2016 edition of this evidence-based document. I don’t want to read depositions in a future lawsuit where the nurses cannot answer basic questions about extravasation and vesicants. To obtain this document, go to https://www.ins1.org/Store/ProductDetails.aspx?productId=241097 to purchase a printed or electronic copy. |
Author: Lynn HadawayLynn Hadaway is an international thought leader in infusion therapy and vascular access, having been in this practice for more than 40 years. Her experience comes from hospital-based infusion teams, device manufacturers, and continuing education services. Her journal and textbook publications are extensive. She also maintains board certification in infusion nursing (CRNI) and nursing professional development (RN-BC). 
Categories
Archives
May 2019
|
||
 RSS Feed
RSS Feed
Copyright © 2020 Lynn Hadaway Associates, Inc. | P.O. Box 10, Milner, GA 30257 | 770-358-7861