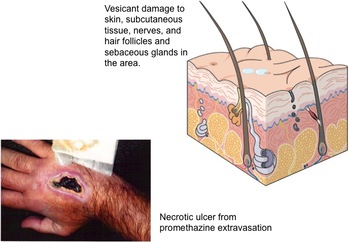
 The growing discussion about the correct use of midline catheters brings up another related issue. What is the definition for vesicant and irritant? What are the differences and similarities? The following definitions are taken from the glossary of the 2011 Infusion Nursing Standards of Practice.
These definitions indicate a major difference of where the damage is taking place. For a vesicant, the damage is occurring in the subcutaneous tissue OUTSIDE of the vein. For irritants, the damage is occurring to the vein wall INSIDE the lumen. Vesicants cause tissue damage that may OR may not require surgical intervention. Notice in the definition the use of the word “or” – blistering, tissue sloughing OR necrosis. Blistering and tissue sloughing are tissue damage but necrosis may not be present. Time is required to heal the area, hopefully without any permanent tissue destruction. Necrosis requires surgical debridement and maybe even skin grafting to allow for complete healing. Vesicants produce this entire range of tissue injury with the damage occurring to the subcutaneous tissue at or near the point of where the fluid is escaping from the vein. This can be at the point of vein puncture or the catheter’s tip location or both. Irritants cause phlebitis (vein inflammation) and thrombophlebitis (thrombus plus inflammation), so the damage is occurring inside the vein lumen. This inflammatory process can produce severe edema but there is no infusing fluid leaking from the vein into the subcutaneous tissue. When peripheral catheters are used for infusion, this is occurring in superficial veins, thus the diagnosis of superficial thrombophlebitis. When it occurs with a PICC or other CVAD, it is most often a deep vein thrombophlebitis. The term, “extravasation” is referring to the leakage of vesicant fluid/medications into the subcutaneous tissue. But this term is not used when the event is from an irritant inside the vein lumen. Signs and symptoms often overlap between these 2 complications. It may be difficult for staff nurses to distinguish the difference and this is where the knowledge and skill of an infusion nurse is required. 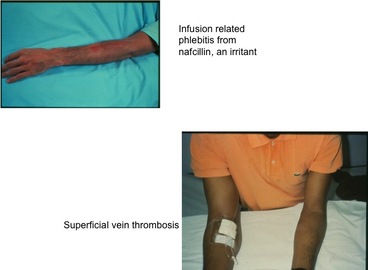
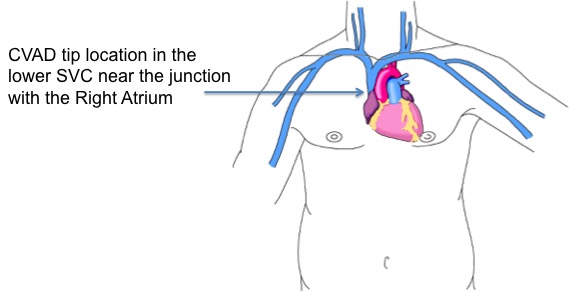 Many healthcare providers are still struggling with the issue of where the tip of central venous access device (CVAD) should be located, including PICCs. It is amazing that this is still being debated but I guess many people have not learned about the evidence of complications associated with suboptimal tip location.
First, where should the tip of all CVADs be located? This would include all percutaneous central lines from subclavian and jugular insertion sites, PICCs, tunneled catheters to implanted ports. The answer comes from many resources. Look at the instructions for use (IFU) for any type of CVAD for the manufacturer’s recommendations for tip location. There are numerous places to find the IFU, a little booklet of critical information that comes in the package with every catheter (inserters find this in the top of the package and it usually goes in the trash!). You can also find this information on the website for many manufacturers. As one example, click here to find IFUs for all catheters made by Bard Access Systems http://www.bardaccess.com/resources.php?category=Instructions%20For%20Use. Also, you can contact your local sales representative or the manufacturer directly to request the IFU for the catheter in use. Carefully read the Warning statements for information about where the catheter tip should NOT be located. Then look at the insertion procedure information for where the tip should be positioned. Most of these IFUs will have a warning statement about avoiding placement in the right atrium and that the preferred tip location is at the junction of the superior vena cava and right atrium. Another important resource is the Infusion Nursing Standards of Practice from the Infusion Nurses Society (INS) with most recent edition published in 2011. The next edition is due to be released in January 2016. Focus on Standard #32, VAD Selection; and #35 VAD Site Preparation and Device Placement. This document definitely states the tip should be positioned in the superior vena cava near its junction with the right atrium. Hemodialysis catheters should be the only CVAD with a tip location inside the right atrium, but the National Kidney Foundation warms that right atrial thrombosis is a serious complication of this tip location. The inserter should be knowledgeable of these recommendations and act accordingly during the insertion procedure. The nurse caring for the patient in the hospital, home care, or any healthcare setting must know where the original tip was located. This information is found in either the post-insertion chest xray or the ECG documentation in the procedure note. Inserters can face challenges when trying to correctly position any CVAD, especially a PICC. But every effort should be made to reach the recommended tip location. If this is not possible, there should be documentation about what was tried to reach the optimal location, the reason(s) for not reaching it, and what was considered before leaving a catheter tip in a suboptimal position. There could be valid reasons for a tip location that is distal to the SVC such as a large tumor encroaching on the SVC, or vein thrombosis such as SVC syndrome, however all subsequent caregivers must be made aware of these issues. Suboptimal positions are known to cause complications including, but not limited to, vein thrombosis due to mechanical trauma to the vein wall; cardiac arrhythmia, and cardiac tamponade with pericardial effusion; secondary tip migration into the jugular vein with retrograde infusion into the intracranial venous sinuses causing neurological complications; and vessel erosion with subsequent infiltration/extravasation into the chest. So your patients are at an increased risk when the tip is not properly positioned. About 15 years ago, concern about the so-called “midclavicular” tip location led the board of directors for the Association for Vascular Access (AVA, NAVAN at that time) to release a position paper on this very issue. Click here to download that paper http://www.avainfo.org/website/download.asp?id=1447 . The body of research supporting the SVC tip location has grown significantly since this paper was published. Check the reference list following each of the Standards from INS for more recent references. Also read Standard #53 on CVAD Malposition. Notice that many of these references are from the medical literature and are not limited to nursing publications. What about the legal ramifications for suboptimal tip locations? Can a nurse or any healthcare professional be named in a lawsuit if the tip is not properly placed? The CVAD tip location alone is not enough to bring about a successful lawsuit. The patient must have damages for a lawsuit to be filed. Complications and patient damages are foreseeable because there are many publications warning about these events and this increases the liability of inserters using suboptimal tip locations. Use of any CVAD with a suboptimal tip location places more responsibility on the nurse caring for the patient. The caregivers must know the anatomical tip location. They also must know the signs and symptoms of these complications so that correct intervention can be done quickly, limiting the amount of damage to the patient. In a legal case, if there was documentation for attempts made to reach the correct tip location and the rationale for allowing it to remain in the suboptimal position, the liability of the inserter may be reduced. Then it would come down to how accurately and quickly the signs and symptoms were recognized and treated by the caregivers. All lawsuits are judged based on the specific details and facts for each case, so there is no way to quantify the risk to the nurse or to predict the outcome of a lawsuit. The best approach is to have a collaborative practice setting where inserters and caregivers work together to make the most appropriate decision for each patient. Policies and procedures are definitely required to guide these clinical decisions. Education for prescribers or other decision- makers is necessary so they have a good understanding of the risk for the patient, all personnel involved and the organization. Each organization must have written policies and procedures for guidance on these issues. Patient protection is paramount to everything else and thus the reason for the recommendations for the CVAD tip location that is known to have the best outcomes. |
Author: Lynn HadawayLynn Hadaway is an international thought leader in infusion therapy and vascular access, having been in this practice for more than 40 years. Her experience comes from hospital-based infusion teams, device manufacturers, and continuing education services. Her journal and textbook publications are extensive. She also maintains board certification in infusion nursing (CRNI) and nursing professional development (RN-BC). 
Categories
Archives
May 2019
|
 RSS Feed
RSS Feed
Copyright © 2020 Lynn Hadaway Associates, Inc. | P.O. Box 10, Milner, GA 30257 | 770-358-7861